Best ACLF specialist in Mumbai & South Mumbai
What is meant by ACLF:- Acute chronic liver failure?
Acute chronic liver failure (ACLF) is a syndrome in people with chronic liver disease, whether they have cirrhosis or not.
Decompensation with liver failure (jaundice and a lengthening of the international normalized ratio) and one or more extrahepatic organ failures are linked to an elevated risk of mortality within 28 days and up to 3 months of the onset.
For a certain proportion of patients, cirrhosis develops naturally throughout the course of chronic liver disease. There are two main stages in cirrhosis. Decompensated cirrhosis begins with the appearance of jaundice, ascites, variceal bleeding, or hepatic encephalopathy; in contrast, compensated cirrhosis is the stage in which none of these consequences appear.
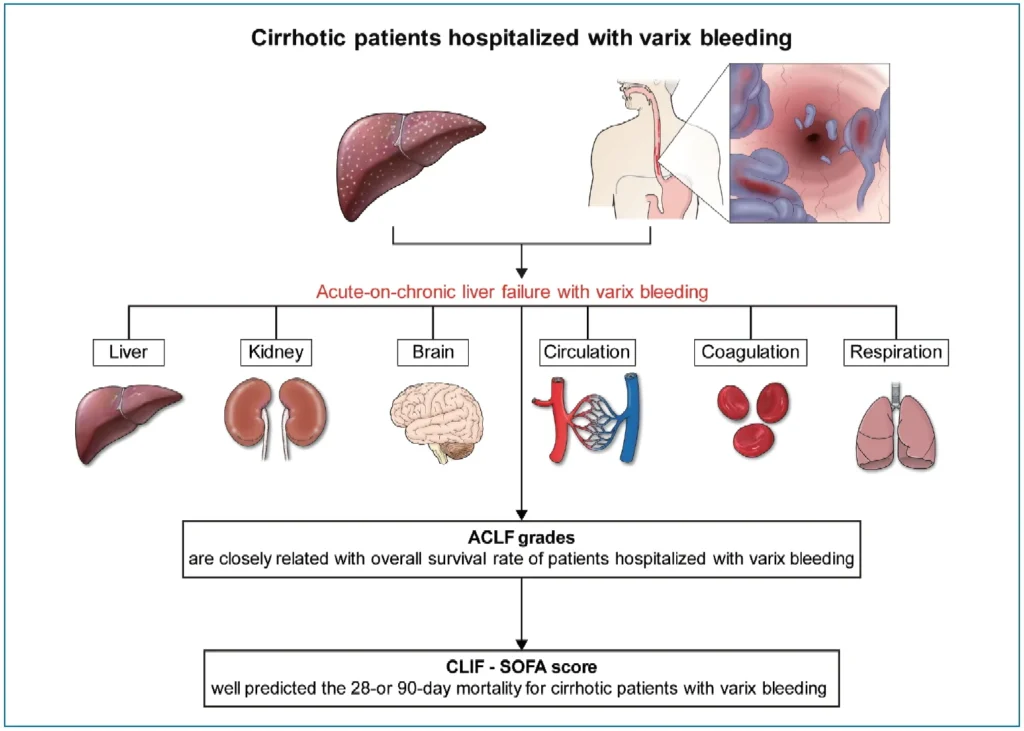
When chronic liver disease, whether present or not, is combined with viral, drug, alcohol, or ischemic hepatitis, surgery, or sepsis
It is possible for the liver disease to progress in either stage of cirrhosis, which could lead to the failure of extrahepatic and hepatic organs. Type A ACLF, Type B ACLF, and Type C ACLF are used to describe ACLF in individuals with chronic liver disease, complex cirrhosis, and decompensated cirrhosis, respectively.
In light of this, advanced chronic liver failure (ALF) is a late stage chronic liver disease involving hepatic and extrahepatic organ failure.
Acute liver failure symptoms and signs might include:
- Your skin and eyes are becoming yellow (jaundice)
- Your upper right abdomen is hurting.
- A bloated stomach (ascites)
- Nausea
- Vomiting
- an overall feeling of being uncomfortable (malaise)
- bewilderment or disorientation
- Sleepiness
- The breath may smell sweet or musty.
- Tremors
At the Institute of Liver Diseases’ Department of Hepatology, Dr. Chetan Kalal is now the Consultant. He is regarded as one of the Best Acute-on-Chronic Liver Failure specialists in Mumbai & South Mumbai. He is a top hepatologist and liver expert. He has received numerous honors, the most notable of which is the coveted AASLD Foundation Award in 2016 and 2017.
Liver illnesses are his main area of research interest. He has spoken at worldwide and national events and published in peer-reviewed journals. He has published more than 20 original pieces in international and national journals. He has also participated in a number of international clinical studies on the development of novel drugs.
A healthy individual may suddenly experience the potentially fatal condition of acute liver failure. Seek immediate medical assistance if you or someone you know experiences any odd changes in mental state, personality, or conduct, as well as any abrupt yellowing of the eyes or skin, soreness in the upper abdomen, or any of these symptoms.